This study was approved by the Institutional Review Board of the University of Colorado, Boulder (Protocol 23-0413). Ten participants (mean age: 27; SD = 3.9; 5 female) took part in this study, all of which partook in all three conditions (Beneficial, Detrimental, and No GVS), in a counterbalanced order. Participants reported no known history of vestibular dysfunction and refrained from consuming alcohol within 6 h prior to the study. Participants were between the heights of 5’2” and 6’3” and weighed less than 225 lbs. as required by the motion device used in the study.
Motion sickness experimental protocol
Participants were outfitted with a 2 × 2” square sponge electrode on each mastoid, held in place with a headband for all conditions (including the No GVS Baseline condition as a sham). Impedance between the two electrodes was checked and found to be below 10 kΩ for all participants. During the first visit, participants received 12 s duration sinusoidal GVS waveforms, of 0.01, 2, and 4 mA while seated on a stool with their feet dangling, back unsupported, arms crossed, and eyes closed to familiarize themselves with GVS and ensure comfort during stimulation. For the experiment, participants sat upright in the TTS, a motion device capable of providing combinations of tilt and translation, with their heads restrained upright by firm foam blocks on each side, which were adjusted to fit the participant’s head. Participants were constrained to the chair by a five-point harness, with arms and legs supported by rigid feet and armrests attached to the chair, located inside a closed chassis that translated along the track. The lights were off to remove visual cues, and white noise was provided in earbuds to help mask auditory cues from the device’s motors.
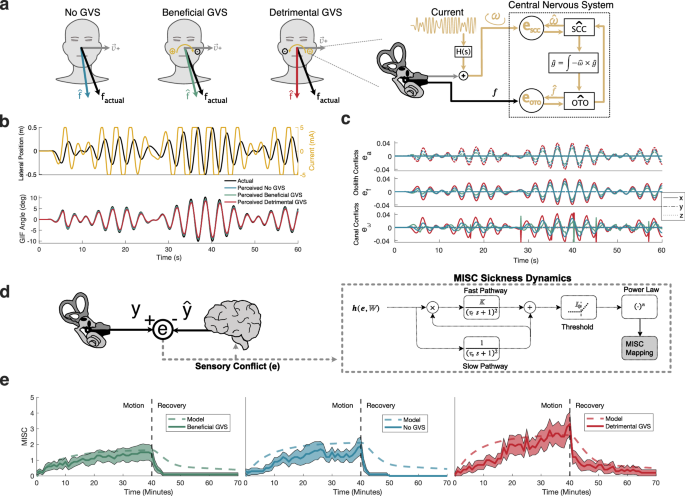
During motion, participants remained upright (i.e., were not tilted) and were linearly translated along their interaural axis (Earth-horizontal) via a pseudorandom sum of sines profile (Fig. 1a, b) for up to 40 min. This lateral translation profile was comprised of low-frequency (0.275, 0.3, and 0.325 Hz) sine waves, and the sum-of-sines translation profile had a peak acceleration/deceleration of ±1.78 m/s2, velocity of ±0.95 m/s, translation of ±0.5 m, and repeating period of 40 s. These motion characteristics were selected to be within the operating bounds of the TTS (particularly for translational velocity and acceleration). A pseudorandom motion profile was selected over a sinusoidal motion profile in order to reduce the potential effects of repeated motion, where participants may be able to anticipate future motions of a repeating single-frequency sine wave motion. Lastly, a lateral translation profile was selected (rather than including roll rotations) to test the hypothesis that lateral translation-inducing motion sickness, where physical motion stimulates only the otoliths, can be altered by GVS, which primarily (and essentially only) influences the semicircular canals. This test provided the opportunity to comprehensively evaluate our understanding of sensory conflict theory and the role of spatial orientation perception in producing motion sickness. Further, lateral translations provided our experiment with an additional degree of ecological validity as lateral translations are experienced in cars, and new patterns of otolith stimulation are experienced during spaceflight, both of which contribute to motion sickness. The same physical motion was administered during all three GVS conditions (described below).
To capture the dynamics of their motion sickness symptoms, before (t = 0), during, and following motion (i.e., recovery), participants continuously reported their motion sickness symptoms using the commonly utilized MISC52 (anchored 0–10 levels; Fig. 4c lists the descriptors associated with levels 1–7, as no subjects reported levels 8–10 before motion was stopped), and this scale has been found to monotonically increase with discomfort during provocative stimulation53. An additional motivation to use the MISC scale is that it is congruent with our computational model output12. Additionally, general discomfort and nausea (on scales of none, slight moderate, and severe) were queried every one minute to further monitor participant comfort and stopping criteria. Two consecutive verbal reports of “moderate nausea” or two consecutive verbal reports of a 7 on the MISC were set a priori as our stopping criterion. These stopping criterion was only reached for one participant, who had an early termination of motion after 39 min of the nominal 40 min of motion during the Detrimental GVS condition. Two-way audio communication and one-way infrared video allowed operators to monitor subjects in the dark. Following the up to 40 min of passive motion, motion sickness reports continued during 30 min of stationary recovery, seated with eyes open in a chair outside the TTS.
Experimental paradigms
Participants (N = 10; 5 female) were randomly assigned in a counterbalanced order to one of the three experimental conditions per visit: No GVS, Beneficial GVS, and Detrimental GVS. To avoid experimental confounds (such as placebo effects) presented by using a No GVS control condition or a different GVS waveform as a sham, the Detrimental GVS waveform was added as a third condition to our experiment in addition to the No GVS condition. The Detrimental GVS condition was identical to the Beneficial GVS waveform, applied with mirrored polarity to the Beneficial GVS current waveform (i.e., reversed polarity electrodes), and predicted to increase motion sickness symptom severity. This approach allowed us to control all other variables between the treatment and sham conditions, keeping the waveform characteristics (e.g., frequency content, time delay, and amplitudes) the same between the two GVS conditions. As a result, the single independent variable between these two conditions is incoming vestibular information alone, modulated by identical GVS waveforms (just with opposite polarity), applied during the exact same physical motion. For the Beneficial and Detrimental conditions, GVS current was applied during the motion phase only, and our GVS device was programmed to start temporally synced to motion as displayed in Fig. 1b. Our GVS device was pre-programmed with the current waveform to enable this sync.
We implemented a within-participants experimental design where each participant experienced each condition over the course of three separate visits (30 total test sessions). Testing within participant groups helps address several statistical complications due to interindividual differences. First, motion sickness is reported subjectively, and interindividual differences in understanding and reporting motion sickness severity using motion sickness scales are expected. Second, there are large interindividual differences in motion sickness susceptibility7,54. Recently in the literature, habituation to repeated motions has been mitigated by spacing testing sessions within participants by at least one week33. Here, each condition was also separated by at least one week (mean: 25 days). A Friedman test of session order revealed no significant effect on MISC rate (p = 0.8).
The GVS waveform administered during the Beneficial GVS condition was predicted to reduce motion sickness during the physical motion profile by nesting simulations of the combined GVS and motion sickness model within an optimization loop (Fig. 5). The first stage of the model enabled quantitatively predicting vestibular sensory conflicts in humans as intermediates of spatial orientation perception during applied passive physical motion and binaural bipolar GVS current24. The second stage of the model weighed vestibular sensory conflicts, both those associated with semicircular canals and otolith organs, to produce MISC symptoms12. The associated weights were trained and validated in a previous study by simulating several passive motion paradigms in the dark with human participant motion sickness reports over time. During the optimization routine, the scalar objective function that was minimized was the predicted MISC after 40 min of the lateral translation motion profile provided to the participants in this study. The optimization variables were weights associated with the GVS current being coupled to a weighted linear combination of physical motion characteristics in the head reference frame (Fig. 5a), including the GIF angle, the time rate of change of the GIF angle, as well as a time delay in the GVS plane. Within the optimization loop, current values above an absolute magnitude of 5 mA were capped at 5 mA to produce current waveforms that would be tolerated by subjects. MATLAB’s fmincon function was utilized to determine the optimal physical motion characteristic coupling. In addition to the results presented herein, this methodology for devising a countermeasure to motion sickness (Fig. 5b) via computational models represents a scientific contribution that can also be utilized to produce GVS waveforms that are predicted to systematically alter spatial orientation perceptions55.
The optimized Beneficial GVS waveform, depicted in Fig. 1b, was proportional to the lateral velocity of the head along the interaural axis. During the dynamic motion frequencies used here, this waveform (coupling factor of 12.7 mA/(m/s)) is tantamount to coupling to the time rate of change of the GIF angle (with a coupling factor of −0.84 mA/(deg/s)) of the head over time given the small GIF angles present in the motion profile. This latter, more robust coupling scheme was developed by enhancing early optimization schemes by modifying the optimization parameters to include a weight/optimization variable on the time rate of change of the GIF rather than the lateral velocity. While these are essentially equivalent (and produce the same model prediction changes in MISC from the baseline simulation without GVS), we encourage researchers to couple applied GVS to the time rate of change of the GIF angle of the head over time for other applications seeking to reduce motion sickness during lateral Earth-horizontal translations experienced along the interaural axis. This physical motion characteristic is robust to prolonged translational velocities, which do not simulate the vestibular system and GVS is likely not needed or beneficial. The translational velocity coupling waveform was used for empirical evaluation and to formulate model predictions throughout this article. Additionally, we provide a means of optimizing/designing any arbitrary GVS waveform that is not coupled to a physical motion characteristic using temporally spaced and splined nodes as optimization variables. This routine and code are included in the linked repository (as well as a comprehensive guide to its construction and implementation56).
Following generating a Beneficial GVS waveform, the Detrimental GVS waveform administered was the polarity-mirrored counterpart to the Beneficial GVS waveform. A priori, the Beneficial GVS waveform was predicted to decrease motion sickness by 22%, and the Detrimental GVS waveform was predicted to increase motion sickness by 23% compared to baseline for the population on average using MISC. A No GVS condition was conducted as a measure of baseline motion sickness without any GVS current applied. However, electrodes were still applied, and participants remained blind to the experimental condition.
Previous studies that have examined GVS as a countermeasure to motion and cybersickness have encountered several notable obstacles. The first is the lack of an obvious sham condition when examining the effects of GVS. In prior experiments, the control condition has simply been only the application of ‘No GVS’21,22,23, in which case participants are likely not blind to the experimental conditions and can likely identify the treatment group given obvious GVS-induced tactile sensations. Further, known side effects of GVS (e.g., tactile sensations, visual flashes, etc.) are confounds in assessing the causal aspects of GVS as a countermeasure, thus the impact of GVS on the vestibular sense alone cannot be isolated. Alternatively, if an alternative sham condition is used instead of a ‘No GVS’ condition, where some other GVS current is applied, then the effects of that waveform (e.g., stochastic resonance, down-weighting of vestibular information, altered tactile cues, etc.) become uncontrolled confounds between conditions. Finally, waveforms used for treatment have been ‘best guesses’ without models of how GVS impacts peripheral vestibular signals, perception, and motion sickness. Our approach of (1) generating a Beneficial GVS waveform computationally for empirical evaluation and (2) evaluating a complementary Detrimental GVS waveform of the same characteristics as the Beneficial waveform, opposite in polarity, enabled circumventing these issues.
With this experimental design, we sought to evaluate the following hypotheses. First, we hypothesized that motion sickness during physical motion will be lower in individuals given the ‘Beneficial’ GVS waveform, computationally predicted a priori to reduce motion sickness via the reduction of vestibular sensory conflict, than in individuals during the same physical motion paradigm given the administration of an equal and opposite, ‘Detrimental’ GVS waveform (computationally predicted a priori to increase motion sickness via the increase of vestibular sensory conflict). Second, we hypothesized that GVS could be utilized in the binaural bipolar configuration to reduce motion sickness symptom severity in the presence of passive, upright lateral translations compared to a control, in which GVS electrodes are worn without current applied.
Statistical analyses
Chosen metrics and statistical analyses were picked a priori from existing motion sickness analyses in the literature that used the verbal MISC reporting metric33,57,58. Motion sickness severity of an experimental condition was quantified using MISC rate: participants’ final MISC report during motion normalized by the time at that report. This metric was chosen as a scalar descriptor of motion sickness severity because it accounts for early termination of the experiment for participants that reached the stopping criterion before cessation of motion, and crucially, because it has been found to be the most discriminative measure of motion sickness for passive motions in the dark and is comparable to other paradigms of varying duration where it has been utilized previously33.
Utilizing the MISC rate metric, we evaluated GVS’s ability to alter motion sickness with a hierarchical, linear mixed-effect model, where each participant is given a random intercept (corresponding to the baseline, No GVS condition) to account for the dependence between observations of the same participant across conditions. This specific statistical analysis has been used previously in the literature to characterize known increases in MISC rate with increasing motion amplitude33. Here, we assess the slope coefficient within this model across a continuous independent variable: the GVS gain supplied to participants during each condition. The GVS gain for the Detrimental condition is −1 (polarity is flipped from Beneficial), the gain on the No GVS condition is 0 (no current is applied), and the gain on the Beneficial condition is 1. Because we predicted a priori that the Beneficial GVS condition would have lower motion sickness than the No GVS condition, which in turn would be lower than the Detrimental GVS condition, we hypothesized a negative slope, resulting from lower MISC rate with increasing gain on the GVS current. Here we utilize a two-tailed analysis, but we note that a one-tailed analysis was justified as a negative slope was predicted a priori.
Using paired t-tests, we then evaluated the individual hypotheses i.e., (1) the Beneficial GVS condition produces less motion sickness than the No GVS condition, and (2) the Beneficial GVS condition produces less motion sickness than the No GVS condition. We confirmed residuals were consistent with being normally distributed. To correct for family-wise error, we implemented a Bonferroni correction (factor of 2, reported as padj) on these tests. Because we had a priori directional hypotheses, quantified using a model of motion sickness with physical motion and GVS current as inputs, we conducted one-sided tests for each. Cohen’s d was used to compute effect size. For post-hoc power analyses, \(\beta\) = 0.8.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.