The screening process for our search is detailed in Fig. 1. Following removal of duplicates between databases, 20,342 unique titles were screened. From these, 19,727 titles were further excluded. Following full text screening, 122 studies were assessed for eligibility, of which 96 were excluded because they had no health-related outcomes (n = 38), were not related to climate change (n = 2), there was no digital technology used (n = 1), not published in English (n = 2), not tested in humans (n = 2), focused on the development or design of a wearable only or did not provide actionable health outcomes (n = 18), used telehealth without the inclusion of health-related outcomes (n = 6), involved the development of an online platform only (n = 16), or were a type of paper excluded from our review (i.e., survey/book chapter) n = 13. This resulted in 24 studies included in the final analysis19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42.

Flow diagram of the review screening process showing the number (n) of studies originally identified, screened, assessed for eligibility with reason for exclusions.
Study Characteristics
A summary of the study locations, year of publication, aim(s), design, and main findings are displayed in Supplementary Table 1. The first articles on record were published in 201236,39. In the following 10 years only seven articles were published, until 2022–2025, where 15 articles were published collectively. When the search was performed on the 11th of March 2025, two articles had been published in 2025 (Fig. 2). Author collaboration clusters are shown in Fig. 3. In total, 123 people authored one document, with five authoring two documents. Publications originated from the United States (n = 5), Germany (n = 2), Italy (n = 2), Japan (n = 2), New Zealand (n = 2), Sweden (n = 2), Australia (n = 1), Canada (n = 1), Chile (n = 1), Finland (n = 1), Indonesia (n = 1), Iran (n = 1), Netherlands (n = 1), South Korea (n = 1) and Turkey (n = 1).

Number of articles and the year of publication for studies included in analysis.
Each cluster represents the group of authors for each manuscript. Where author collaboration exists, the thickness of the line between clusters represents the strength of the collaboration. However, our analysis found no collaboration between any authors who have published from the included articles.
Table 1 shows the outcome measures and digital technology used within which climate change topics, categorized into either health outcomes, health education, behavior change or implementation. The areas of interest were using digital technology to improve health education (n = 11 studies), modifying health outcomes (n = 9 studies), followed by altering health behavior (n = 6 studies) and implementation (n = 7 studies). Three studies used co-design in the development of their technology24,25,37, 12 studies used their technology to prepare people for extreme weather events (i.e., flood or earthquake evacuations)19,20,21,22,23,25,26,27,28,29,30, and six studies used technology to help people manage their health during extreme weather events25,33,35,36,37. Digital technologies used (with some studies using more than one) included virtual reality (VR; n = 9), smartphone application (n = 7), gaming (n = 7), online platform (n = 4), wearable (n = 3), telehealth (n = 2) and text messaging (n = 1).
Study participants
Twenty-three of the 24 studies reported participant information. There was a total of 18,749 participants. Nineteen articles included information about participant sex, and from those, there were a total of 1533 participants: 703 (45.9%) were male, 825 (53.8%) were female, three were non-binary (0.2%) and two (0.1%) preferred not to specify their sex. The age of participants reported from 12 studies was 36 (7–87 years). Participant demographics ranged from primary and secondary school and university students to farm workers, people with diabetes and chronic obstructive pulmonary disease (COPD) and general population residing in the area where the study was undertaken (Supplementary Table 1).
Study design
Seven studies employed various smartphone app-based interventions targeting health education/preparedness for and management of health outcomes (e.g., heat-related illness) during climate events. In some studies, the efficacy of the app was compared to ‘standard care’34,38 or control conditions without the use of an app25,30. Four studies used pre and post-questionnaires to assess the effectiveness of an intervention on health education31, or modify behavior or decision making34,38 employing either a within- or between-subject design. Other studies used apps to improve decision making, such as improving evacuation times during a tsunami by assessing the time to evacuation30 or monitoring biometrics and/or predicted thermal stress (two in the heat25,35 and one in the cold27) and providing actionable advice to remain in a healthy thermal state.
Nine studies used VR to understand the influence of immersive experiences to improve health education, climate change health-related awareness and modify behavior. Virtual reality was primarily used to prepare individuals for making decisions during climate events, with seven of the nine studies serving this purpose. In several studies, the effectiveness of exposure to VR or 3D simulations was compared to traditional information delivery methods, such as PowerPoint, or control conditions without VR22,23,29,42. Study designs mostly used pre- and post-test questionnaires to measure knowledge, attitudes, self-efficacy, and intentions. In most instances, the duration of VR engagement was not reported, however, in those studies that did, durations varied from 60 s to ~30 min. Several studies utilized immersive narrative experiences or interactive tasks where participants’ actions within the VR environment affected the outcomes they observed, particularly during VR that simulated evacuations. The study designs commonly incorporated elements of inquiry-based learning, multimedia, and gamification to engage participants and assess both cognitive and emotional impacts.
Digital technologies often employ gaming to improve health education and behavior using pre and post-test questionnaires, with most users engaging in the game once. The design of games varied, and was used through either VR or online platforms, including some specifically purposed for educational settings, which improved players’ knowledge about climate change and their decision-making abilities. Other games emphasized feedback to reinforce learning20, or incorporated storytelling elements41 to increase both knowledge and engagement. Game durations varied widely, ranging from a single 25-minute session to several weeks of gameplay. However, the length of time spent playing did not appear to significantly impact outcomes, with enjoyment and positive emotions toward climate change remaining consistent across different gameplay durations.
Three studies used wearables to measure human physiological and environmental parameters to improve health outcomes and education and modify behavior25,32. All studies employed a feedback system where people would become aware of their health status or surrounding environment based on the wearable and behaviors were monitored accordingly.
Two studies utilized telehealth interventions: one delivered eight weeks of cognitive behavioral therapy to alleviate climate-related anxiety40, while another provided nine months of remote monitoring for patients with COPD33, aiming to reduce exacerbations during hot weather. The telehealth platforms facilitated regular check-ins, remote consultations, and personalized feedback. Both studies demonstrated that telehealth interventions were significantly more effective than control groups, improving patient outcomes by providing continuous care, timely interventions, and tailored support.
Four studies used online platforms. Online platforms were used for a range of purposes, including tracking health symptoms36, improving mental health39, and improving health education and decision making24,41. The duration of engagement with the online platforms ranged from a single 45 min session, to 60 days of use. These platforms incorporated features like real-time feedback, interactive modules, and progress tracking to enhance user engagement. Whether focused on symptom logging, or behavior change, the platforms were effective in achieving their objectives by improving learning outcomes and influencing positive behavioral shifts.
One study used a text messaging intervention37. Text4Hope employed daily supportive text messages across a 3-month period, designed on behavioral cognitive therapy to reduce symptoms of depression and anxiety and improve resilience and well-being during the wildfires in Canada. This study incorporated baseline and post intervention questionnaires demonstrating improvements in wellbeing, anxiety and resilience.
Study outcomes
Outcome measures for the included studies were classified into health outcomes, health education, behavior, and/or implementation. Figure 4 depicts the outcomes measures and effectiveness of digital technology to achieve the aim of each selected study, with some studies utilizing multiple outcome measures.
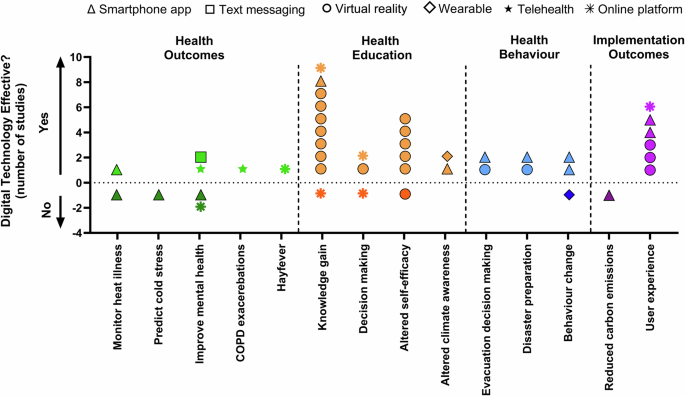
Health outcome measures are presented in green, health education in orange, behavioral outcome measures in blue and implementation outcome measures in purple. Dark colors indicate that digital technology was not effective at achieving that outcome measure, light colors indicate it was effective. The dashed line denotes effective interventions and dark colors below the dashed line denote ineffective or detrimental interventions. Symbol types depict different technologies employed, specifically smartphone apps (triangles), text messaging (squares), virtual reality (circles), telehealth (pentagonal stars), wearable technology (diamonds), and online platforms (octagonal stars).
Nine studies used digital technology for health-related outcome measures. The primary aims of these studies were to: monitor heat stress (n = 2), predict cold stress (n = 1), reduce COPD exacerbations during heatwaves (n = 1), reduce hay fever symptoms (n = 1) and manage/improve climate change-related mental health challenges such as depression, anxiety, coping or quality of life (n = 4). Studies utilizing wearables improved awareness and data collection but had limited impact on behavior change and heat stress detection25,32. Smartphone apps were both ineffective at monitoring heat illness25 and predicting cold stress27. Telehealth was effective at reducing COPD exacerbations33 during heatwaves, and an online platform where people could receive information/monitor their allergies was effective in reducing people’s hay fever symptoms36.
A 3-month text-based program (Text4Hope) used during the Canadian wildfires and an internet-based cognitive behavioral therapy program showed improvements in wellbeing, depression, anxiety and post-traumatic stress disorder symptoms37. Conversely, a web-based platform used to reduce depression and anxiety symptoms and improve coping during hurricane Ike, showed no improvements in any mental health outcomes measures except mitigating symptoms of worry39. Similarly, a mobile app aimed at improving prenatal environmental awareness was beneficial at improving health behaviors, but did not improve symptoms of depression or anxiety34.
Eleven studies assessed the use VR (n = 7)20,21,22,26,28,29,42, online platforms (n = 2)24,41, wearable (n = 1)25 and a smartphone application (n = 1)31 to improve health education. In almost all studies, digital technologies were effective at improving knowledge gain and self-efficacy about specific topics of interest. Topics ranged from learning the signs of heat stress and mitigation strategies22,25, safe evacuation strategies during earthquakes20,21,28,29 to learning how to prepare for and protect oneself during wildifres24. Only one study demonstrated no increase in self-efficacy following a VR simulation to improve earthquake evacuation safety29.
Six studies used digital technology to alter behavior and/or improve decision making (Fig. 4). Some studies used digital technology to alter how people respond to and/or the time it takes to make a decision and effective evacuation strategies for disasters, such as tsunamis, floods and hurricanes19,23,30. For these studies, digital technology was effective in improving behavioral responses to emergency situations. Smartphone apps were also used for behavior change and were effective at changing people’s diet behaviors38 and environmental health behavior34, yet demonstrated no change in motivation or intention to change travel behaviors despite increased awareness of their surrounding air pollution32.
Seven studies assessed the efficacy of digital technology implementation. The main outcomes for implementation were user experience (n = 6) and reduction in carbon emissions (n = 1). In all studies, the use of digital technologies had high satisfaction for user experience. One study used education through an app to change people’s diet choices and ultimately reduce greenhouse gas emissions from food waste but showed no reductions in greenhouse gas emissions (Fig. 4, Supplementary Table 1).
Semantic analysis of abstracts
Supplementary Fig. 1 is a visual depiction of the semantic analysis of abstracts of included studies. Clusters are indicative of the strength of association between words. Cluster 1 (purple, ten items) focuses on climate change and sustainability. Cluster 2 (dark blue, ten items) focuses on types of study and outcomes like virtual reality, knowledge and self-efficacy. Cluster 3 (green, seven items) focused on heat and wearables. The term ‘intervention’ was the most frequently used in all abstracts.