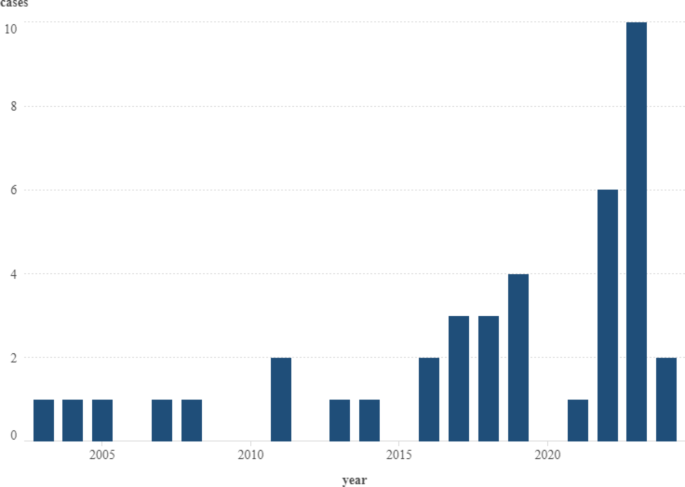
Human alveolar echinococcosis is an increasing health problem in Hungary. Between 2003 April and 2024 April, 40 cases were detected, of which 25 entered the health care system during the last 5 years. Two hyperendemic foci are supposed to form in the country, one in the Northern Hungarian Mountains, and another in the southwestern part of the country, the South Transdanubia. The period prevalences for these focus areas, 9.46/105 and 23.07/105, are similar to those, which were detected in the previously identified highly endemic regions close to the historical Alpine focus area2.
Cluster analysis by SaTScan software could detect a high-risk and a low-risk HAE cluster in the eastern part of the country while the South Transdanubian case accumulation remained non-detected by this method. The Bernoulli-based approach uses the presence of cases in a district as a quality regardless of the prevalence in the district concerned. The South Transdanubian case accumulation involved only four districts as a contiguous area, and three districts further with plenty of negative districts around these spots, therefore the software identified this phenomenon as a coincidence.
The spatial rate smoothing could highlight the potential risk of HAE in the South Transdanubia, which remained undetected by cluster analysis. In the case of foxes, the smoothing process displayed a pattern that agrees with the strong hypothesis that E. multilocularis spread to Hungary from the northwest direction14. Smoothed risks of both HAE and fox echinococcosis removed the least risky classification from the Great Plain districts. This procedure can provide a more appropriate estimation of risk than use of crude proportions, especially when the sample is not optimal to represent the whole population at risk15. Therefore, increased smoothed risk within the apparently free area reflected the possibility of disease occurrence.
For analyzing those variables that could influence the smoothed risk of HAE in a district, we applied the MGWR model, which could handle the heterogeneity of the candidate explanatory variables. The model provided a high R2 values (0.459–0.866) for almost the whole territory of the country, except for the southernmost areas of the Great Plain where the fitness of the model was moderate. The model detected two factors which affect HUMRISK globally. The socio-economic factor (DDI) showed negative influence on HUMRISK, thus less developed districts represented higher risk for HAE. Forest cover proportion of the district (FOR) also prevailed globally but with a positive influence, whereas the more the forest cover caused the higher the risk of HAE.
Those variables, which were involved as previously proven drivers of E. multilocularis endemics, such as earth skin temperature, ground surface wetness, and infection prevalence in red foxes2,16, showed various impacts on HAE by regions. In the northern part of the country, which was reached by the parasite for the first time14, both the soil temperature (TSMEAN) and the smoothed prevalence in foxes (FOXRISK) behave very similar as it was detected within the historical focus of E. mutilocularis16. On the other hand, the moisture content of the ground did not show a significant impact on the smoothed period prevalence of HAE (HUMRISK) here.
The Northern Hungarian Mountains are under a strong influence of continental climate, which is modified by the microclimatic effect of the relief. This complex climatic impact causes harsh winters but less hot and dry summers in the mountains than in the surrounding plain areas.
Although the North Hungarian Mountains have a more humid climate than of the Great Plain, both showed the same pattern in correlation between ground surface wetness and HAE risk. The bandwidth for the humidity of the soil surface (GWTOP) proved large, thus this variable prevails in large areas. Besides the direct linkage between the two regions, a remarkable west-to-east change to a more continental climate can explain the similar GWTOP effect of the North Hungarian Mountains and the Great Plain. The controversial relationship between soil surface humidity and HAE prevalence apparently questioned the previously proven impact of humidity on HAE risk. Nevertheless, it is worth noting that our study investigated district level values of different variables, therefore it was not suitable to detect microfoci within the concerned district. However, these small habitat spots can be the keys in the transmission of E. multilocularis17.
The South Transdanubian Region of Hungary is affected by sub-Mediterranean climatic impact18. Hot summers and mild winters are very different from the climatic features of the historic focus of E. multilocularis19. In spite of this difference, a remarkable case accumulation could be observed in this area, especially during the last five years. Moreover, neither the comprehensive surveillance that was carried out in the red fox population of the region could provide an explanation for the phenomenon20. In the western part of this area both the skin surface temperature and soil humidity showed a negative effect on smoothed period prevalence of HAE, thus the warmer the temperature and the lower the humidity resulted in the higher the risk of HAE. Moreover, on a spot inside this area, a HAE case accumulation in humans accompanied by a low prevalence in red foxes.
It is less probable that the E. multilocularis population in the southern part of Hungary differs this rate in its environmental demands from the northern populations. Though, genetic studies proved that the Hungarian E. multilocularis population has a higher genetic diversity than of Slovakian or Czech populations, the origin of all Central Eastern European populations are proved to be the historical focus in the Alps21,22.
A possible explanation for the parasite’s apparent preference for unsuitable district level environmental conditions could be a compensatory mechanism by other factors. These factors can also prevail in microfoci, in which the optimal conditions of survival and transmission exist in spite of the generally existing suboptimal climatic conditions. These factors can be detected by micro-epidemiological investigations, which can disclose local risk factors10,17. Another reason for the parasite’s success in less appropriate conditions is the presence of regionally prevailing factors, which compensate for the risk mitigation effect of the suboptimal climate.
In South Transdanubia, this risk raising factor can be the composition of the predator community in this region, which is characterized by a large density of golden jackal (Canis aureus) populations. This wild canine can carry E. multilocularis and can significantly increase the risk of HAE in smaller geographical habitats. In South Transdanubia, the stable presence of golden jackals modifies the risk caused by foxes. These two mesocarnivores strongly compete for sources, thus resulting in increased occurrence of foxes around human settlements because they can tolerate humans better than golden jackals do23,24. Besides competition and spatial distribution of these two canids, dissimilar host suitability might enhance each other’s role in disease transmission1,25.
The other, district level, factors that could affect the prevalence of HAE are DDI and FOR, which have the same impact in both hyperendemic focuses of HAE. It is curious that both the socio-economic factor (DDI) and forest coverage (FOR) level had homologous effects in each investigated district, though with opposite signs. Between DDI and FOR variables, the statistical analysis could not identify multicollinearity, therefore both factors have their own impact on HAE risk in humans.
In the case of forest coverage, other research resulted in various conclusions. Most studies concluded that mature forest stands with high biodiversity provide less suitable habitat for E. multilocularis spread than meadows or shrublands, which are generally agreed as the most hazardous habitats for maintenance of E. multilocularis2,5,26. In our research, the applied data source did not distinguish between different types of forests, e.g. shrublands or woody pastures, thus the exact risk of different sylvatic environments could not be identified.
In Hungary, extended grasslands are characteristic exclusively for the Great Plain27, which proved quite the less risky area of the country. On the other hand, smaller patches of grasslands are very important natural habitats in both the Northern Mountains and in Transdanubia28. In Hungary, the proportion of true grassland area decreased for two reasons. On the one hand, human demands for area, such as urbanization and intensification of agriculture, reduced the area of grasslands. On the other hand, the end of extensive animal farming resulted in reduced pasturing and mowing activity, which led to afforestation of pastures and meadows27. For this reason, we presumed that a high proportion of forests at a district level meant a higher proportion of natural habitats compared to urban areas and large-scale arable lands. Our finding that forest coverage was identified as a general risk of HAE agreed with the early findings within the historical focus, thus mainly rural environments carried high infection risk2.
For infection with HAE, a higher risk of low-income regions and low education level was investigated in China3,29 and Kyrgyzstan4. All studies emphasize the importance of individual knowledge on prevention. In our study, the education level groups of the patients were exactly equal, whereas one third of the patients had low, intermediate, and higher education levels, respectively. Therefore, the individual’s educational level apparently did not affect the chance of infection. However, the socio-economic environment seemed to have a strong impact on the patients’ risk for HAE acquisition. A district’s development index depends on a list of factors, which determine access to information, healthcare, and services. The central role of an appropriately functioning and achievable healthcare system in prevention and early diagnosis could be well illustrated in Kyrgyzstan studies. After the end of the Soviet Union, the collapse of the local healthcare system led to the dramatic increase of both cystic echinococcosis, which is caused by E. granulosus, and HAE cases4.
The questionnaire survey was based solely on the interrogation of diseased people. Therefore, in the lack of a control group, it was not suitable to determine relative risk of different potential risk factors but frequency of occurrence of these factors in cases. The questions involved in the survey were adapted from a previously performed study30. Our survey revealed that 66.67% of HAE patients engaged in kitchen gardening. Thus, this lifestyle element was the most frequently chosen one among the respondents. This finding agrees with the experiences of a case-control study completed in Germany31.
A European large-scale study on food self-provisioning revealed that the central motivation for gardening is financial as the poorest social groups produced a part of their food demand32. The questionnaire did not ask directly about the financial background of the respondents, therefore gardening as a socio-economic indicator of limited income could not be proven by this study. Moreover, less developed districts are characterized by countryside abandonment all over Europe33. This phenomenon creates plenty of appropriate, undisturbed shelters and feeding sites for mesocarnivores, such as red foxes and golden jackals, in the surroundings and inside the human settlements. Less sufficient waste management, which is also common in poor regions, provides a huge number of anthropogenic sources for survival and successful breeding of wildlife34. In densely populated fox habitats, even lower prevalence of E. multilocularis can generate a higher risk as it could be observed in Switzerland between urbanised foxes2.
The presence of golden jackals in the less developed districts in South Transdanubia highlights an anomaly, which could be experienced in the relationship between the soil surface temperature and HAE prevalence of a district in the eastern part of the region. In spite of very similar characteristics to the western part of the region, the eastern half seemed free from HAE. Therefore, only spatial rate smoothing suggested suspicion of risk eastward in South Transdanubia. However, the complete lack of cases in the southernmost districts of the east reversed the positive association between soil temperature and HAE risk, which was identified in the west.
The anomalous districts are part of Ormánság (Supplementary Information 1), one of the poorest regions in Hungary. The average inhabitants are characterised by low education and consequential low income, without vision and ability of self-care35. Considering these facts and the biotic and climatic similarity of this region with the neighboring HAE focus, it cannot be excluded that the apparent freedom of this area is due to the locals’ inattention. During the disease course, initially, the clinical signs of HAE are lacking or less severe36,37, therefore most patients do not suspect a life-threatening disease. In addition, disease prevention and health screening tests do not fit the culture of poverty, which characterize the small villages of Ormánság35. Our lack of confidence in the disease-free status of Ormánság was supported by the study of Balen Topic et al.38, which detected a HAE case accumulation in Croatia, not far from the southern border of Ormánság. The contradictory finding about the southeastern part of Transdanubia highlighted the paramount importance of knowledge dissemination not only in known hyperendemic focuses but areas with uncertain status.
In this study, we investigated the interdependence of potential influencing factors and E. multilocularis infection in humans and foxes. For statistical analysis, we applied geospatial methods to determine the risk of HAE and its background at a district level. As a result, we revealed that two, very different HAE foci have been localized in the country, yet. However, the driving forces of HAE in the two foci proved remarkably different. The Northern Hungarian Mountain focus was found to be similar to the historic focus of E. multilocularis in the Alps19,26. This observation agrees with the studies implemented in Czechia and Slovakia where E. multilocularis prevalences in foxes39,40 and in humans16,41 are proved to be high. In the northern focus, cool soil temperature and higher parasite prevalence in red foxes seemed to increase the risk of human infection at district level. Curiously, humidity as a risk factor could not be justified, which contradicted the previous study results that confirmed the humidity dependence of E. multilocularis40,42.
The South Transdanubian focus showed a very different risk pattern. Warm and dry soil surfaces appeared to have higher HAE risk than a humid and cool environment. Based on this apparent contradiction to known environmental demand of E. multilocularis19,26, we concluded that other, not investigated factors enhanced the disease transmission within this area, in spite of the suboptimal climatic features. This observation draws attention to the significance of micro-epidemiological investigations, which can identify microfoci and their risk factors contributing to HAE transmission even in seemingly less appropriate conditions10,17,42.
Our study recognized an area in the country, which behaved in the model as an anomaly. This area is one of the poorest zones of Hungary. The climatic and biotic characteristics of this area is very similar to the neighboring South Transdanubian focus and a Croatian area with HAE accumulation10,38,42. In spite of that, HAE has never been detected here. We concluded that without comprehensive knowledge dissemination and health screening of the inhabitants, this anomaly cannot be evaluated correctly, and the status of this area remains uncertain.
Our study possesses limitations, which mostly originated from the spatially aggregated distribution of the few confirmed HAE cases. However, the geospatial analysis of the known cases denoted two hyperendemic foci of the disease with apparently free areas around them. Based on this finding and the data of the surrounding countries, we deem that the recently seen data are incomplete and cannot describe the true situation. In Slovakia16 and in Croatia38, 137 and 6 HAE cases were detected, resulting in an annual incidence of 0.187/105 and a prevalence of 4.91/105, respectively. Both recently determined hyperendemic foci are located adjacent to similar HAE hot spots of the neighboring countries. This geographical vicinity suggests a cross-border connectivity of the endemic areas. Therefore, the diagnostic sensitivity of the healthcare service of Hungary needs improvement. The apparently increasing annual incidence, especially in the last five years, may also indicate that the early inefficiency of the diagnostic system is in a slow transition towards enhancement. The rapidly changing diagnostic efficiency cannot make sense of calculating annual incidence of HAE, which could suggest an intensively worsening epidemiological situation. Though we cannot exclude even this possibility, in this stage of the research, we hypothesize that raising disease awareness of healthcare professionals caused the apparent increase of annual incidence of HAE.
Another shortcoming of the study was that only 28 patients could take part in the questionnaire survey. Moreover, a control group was not interrogated parallelly with the case group. For this reason, the results of the survey could highlight potential risk factors without determination of relative risk. However, the factors that were chosen most frequently by the respondents of our study, such as gardening and dog ownership, are those which were determined by a previous case control study as the most important risk factors31.