Network structure and central nodes
This section provides a global overview of the pain-related lexical network, focusing on its structural scale, density, and community structure derived from 123,840 word co-occurrence relations. The resulting network comprises 5630 nodes and 86,972 edges, where each node represents a word and each edge denotes co-occurrence4,8,9. Terms such as burning, headache, discomfort, and ache exhibit prominent connectivity, suggesting frequent semantic associations.
Figure 1 illustrates a core–periphery structure: larger central nodes reflect higher centrality and discourse influence, while peripheral nodes reveal the stratified nature of pain-related language11,12.
Fig. 1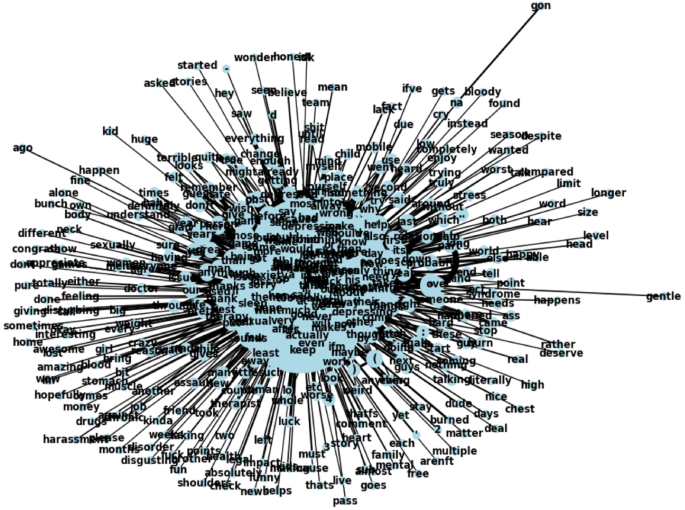
Network visualization of pain-related terms. Co-occurrence network of 5,630 unique terms and 86,972 edges. Nodes represent individual terms; edges represent co-occurrence within a five-word sliding window. Node size scaled by centrality values. All nodes displayed in uniform color.
Although sparse in overall density (0.005500), the network displays high local connectivity. The average degree is 30.900000, indicating that each term connects to roughly 31 others13. The network diameter is 5, suggesting even distant terms are linked via short paths, supporting efficient semantic flow14.
The clustering coefficient of 0.770000 confirms that words form tightly connected local subgroups15. Louvain community detection identified 12 distinct communities16, with the largest including 1,021 nodes and others containing 911, 842, 520, and 495. These findings indicate a globally cohesive structure with semantically distinct subgroups reflecting thematic and contextual variation.
Structural roles of pain-related terms
This section focuses on identifying the lexical roles and relative centrality of individual symptom-related terms within the network. Figure 2 shows centrality metrics for key pain-related terms and their co-occurrence patterns. The analysis revealed a structured subgraph of 309 nodes and 363 edges11,12, capturing the complexity of symptom language on social media, including both frequent and unique word pairings.
Fig. 2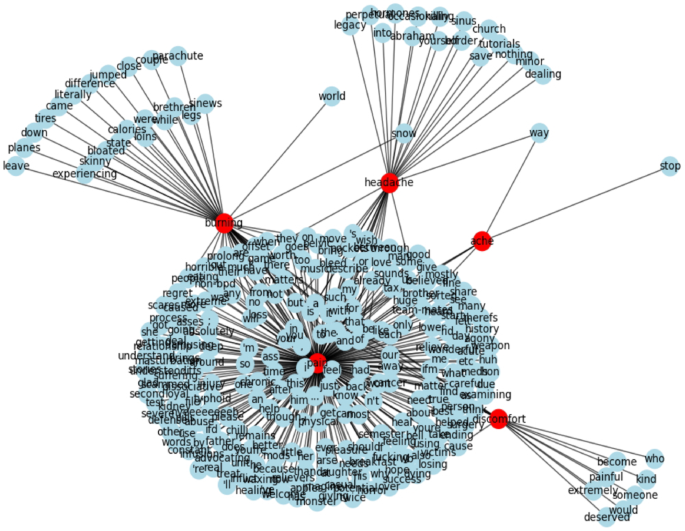
Centrality measures for key pain-related terms in the network. Red nodes: primary pain-related keywords (pain, headache, burning, discomfort, ache). Blue nodes: secondary terms connected via co-occurrence. Node size proportional to degree centrality. Edge length inversely related to co-occurrence strength; shorter edges represent stronger associations.
The term pain consistently scored highest across all three centrality metrics—degree (0.821429), betweenness (0.930134), and eigenvector centrality (0.695893)—indicating its dominant role in organizing and connecting discourse elements across the lexical network13,15,17. In contrast, terms such as headache (0.107000, 0.109000, 0.055000), burning (0.182000, 0.166000, 0.110000), and discomfort (0.049000, 0.052000, 0.024000) displayed substantially lower scores, pointing to a pronounced structural hierarchy.
Notably, contextual analysis using the GoEmotions corpus showed that burning co-occurred almost exclusively with metaphorical or aesthetic descriptors (e.g., glass, carving), rather than with emotion- or symptom-oriented terms, suggesting a more figurative usage pattern.
Beyond individual terms, we examined centrality patterns across broader categories of pain—neuropathic, somatic, visceral, and psychosomatic—using a lexicon-based classification. Of the 21 predefined terms, only 6 (28.6%) were found in the co-occurrence network. Among them, psychosomatic terms such as depression and anxiety exhibited the highest eigenvector centralities (≈ 0.710000), indicating central placement in semantically influential regions. In contrast, clinically salient neuropathic terms like burning and shooting had lower connectivity and minimal network influence (e.g., burning ≈ 0.000000000000013). Somatic and visceral descriptors were largely absent, with only pressure marginally represented.
These findings reveal an asymmetry in how different pain modalities are linguistically expressed: while affective and cognitive terms dominate the discourse structure, physiologically grounded vocabulary remains peripheral or omitted. Full metrics by category are provided in Supplementary Table S1.
Statistical profiling of centrality in the pain network
This section presents a statistical characterization of centrality patterns among symptom-related terms, with the aim of evaluating structural hierarchy and connectivity within the lexical network. The pain-focused network exhibits a sparse but semantically ordered structure, with a density of 0.005500. The average degree is 30.900000, indicating that each node is connected to approximately 31 other terms on average. The network diameter is 5, meaning that even the most distant nodes are linked via relatively short paths, enabling efficient semantic propagation13,14.
Centrality analysis identified pain as a pronounced hub node, with markedly higher values than all other terms in degree centrality (0.821429), betweenness centrality (0.930134), and eigenvector centrality (0.695893)13,15,17. These values indicate an integrative function across the network. Figure 3 presents a logarithmic histogram of these three centrality measures, highlighting the dominant position of pain in contrast to terms such as headache (0.107000, 0.109000, 0.055000), burning (0.182000, 0.166000, 0.110000), and discomfort (0.049000, 0.052000, 0.024000); ache also displayed similarly low scores (not shown in the figure).
Fig. 3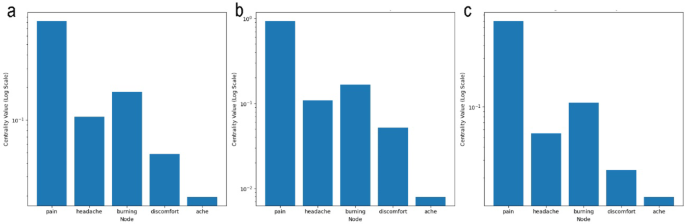
Logarithmic histogram of centrality measures for key pain-related terms. (a) Degree centrality. (b) Betweenness centrality. (c) Eigenvector centrality. Terms: pain, headache, burning, discomfort, ache. X-axis: node labels. Y-axis: centrality values (log scale). Each bar represents a node.
Figure 3a shows degree centrality, which reflects the number of direct lexical connections maintained by a node. Pain exhibits the highest value, indicating its role in anchoring extensive semantic associations within the network. In contrast, headache and burning maintain fewer but still moderate links, while discomfort and ache are sparsely connected, reflecting their marginal connectivity.
Figure 3b highlights betweenness centrality, which measures how often a node lies on the shortest paths between other nodes—indicating its function as a bridge across semantic subgroups. Here again, pain dominates, suggesting that it facilitates cross-cluster discourse integration. Burning and headache display lower but nontrivial betweenness values, implying partial bridging roles. Meanwhile, discomfort and ache are nearly absent from these connective pathways, underscoring their peripheral status.
Figure 3c quantifies eigenvector centrality, which evaluates a node’s influence based on its proximity to other highly connected terms. The figure shows that pain holds a privileged position within the semantic core, exerting influence through its connections with other central terms. Burning ranks second in this metric, although it remains substantially lower than pain. In contrast, headache, discomfort, and ache display lower and more stable eigenvector centrality scores, indicating that they are situated in more context-specific and structurally marginal positions.
Together, these visualizations reinforce a clear structural hierarchy: while pain anchors the network’s core, other symptom terms form secondary or peripheral nodes, playing more specialized roles within constrained lexical contexts.
Each centrality metric offers a unique interpretive lens: degree centrality reflects the number of direct connections, betweenness centrality captures the term’s bridging role between semantic clusters, and eigenvector centrality quantifies influence within densely connected regions. These distinctions illuminate the functional heterogeneity of symptom vocabulary. While pain anchors the structure by linking diverse terms and domains, other expressions such as headache and burning occupy more context-dependent and localized roles.
Community structure in pain discourse
This section presents an analysis of how symptom-related terms cluster into semantically coherent communities, building on the centrality results described above. Based on Louvain modularity analysis, we examine whether structurally prominent terms like pain anchor broader thematic clusters, and how other expressions organize into distinct experiential or symbolic subdomains.
As shown in Fig. 4, the network is divided into multiple color-coded communities. The largest, labeled Community 2, contains 225 nodes and functions as a central hub of general pain discourse. Its average degree centrality is 0.007100, betweenness centrality is 0.004500, and eigenvector centrality is 0.046400. These values suggest that this community not only exhibits dense internal connectivity but also acts as a semantic bridge across other subgroups. With an average edge weight of 5.906200, terms in this cluster tend to co-occur frequently, reinforcing their mutual contextual associations.
Fig. 4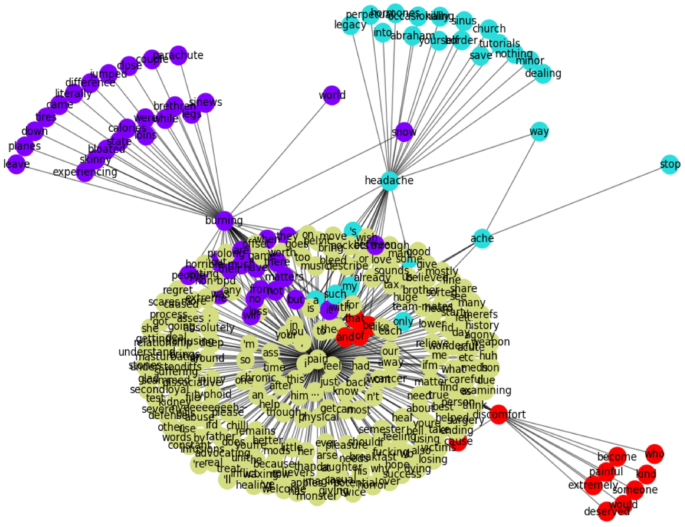
Detected Communities in the Pain-Related Network Using the Louvain Method. Community structure of the pain-related lexical network, based on Louvain modularity detection. Each color denotes a distinct community. Community 0 (light blue): cluster around headache, including both literal symptom terms (e.g., sinus, minor) and metaphorical expressions (e.g., border, legacy). Community 1(Red): centered on discomfort, including relational and evaluative terms (e.g., who, would, deserved). Community 2 (yellow): largest cluster (225 nodes), centered on the term pain, representing general pain discourse. Community 3 (purple): cluster anchored by burning, combining somatic (e.g., legs, bloated) and symbolic terms (e.g., regret, church). Node size corresponds to degree centrality. Edge length inversely proportional to co-occurrence frequency.
The presence of additional, smaller communities reflects the thematic diversification of pain-related expressions. For example, Community 0, with 44 nodes and an average degree centrality of 0.008900, likely represents a moderately connected but distinct conceptual subgroup. Community 3, consisting of 14 nodes, stands out for its relatively high betweenness centrality of 0.009000, implying a mediating role despite its small size.
Close examination of the semantic profiles of specific communities reveals how pain-related terms are framed across experiential, emotional, and symbolic dimensions. One community, colored red and centered around the term discomfort, includes primarily relational and evaluative expressions such as who, would, and deserved. This linguistic configuration suggests that discomfort is often articulated in interpersonal or normative contexts, rather than through direct sensory description. Another cluster, shown in light blue and structured around headache, contains both symptomatic terms like sinus and minor, and systemic or metaphorical ones like border, legacy, and outsource. This distribution highlights the dual semantic role of headache, functioning both as a literal symptom and as a metaphor for social or cognitive burdens.
A third notable cluster, represented in purple and organized around burning, integrates terms with somatic references—such as bloated, legs, and skinny—alongside words associated with emotion, society, or spirituality, including regret, church, and world. This blend illustrates the polysemous character of burning, which serves as both a physiological descriptor and a symbolic or emotional expression in discourse.
Taken together, these findings indicate that social media users construct pain not only as a physical sensation but also as an emotionally charged and morally situated experience. The network structure shows that linguistic representations of pain diverge across bodily, emotional, and social registers, yet often reconnect through central terms that bridge these domains. This pattern of differentiation and reintegration underscores the complexity of symptom discourse in online contexts.
Structural centrality of pain compared to emotion-related terms
This section presents a comparative analysis between pain and emotion-related terms, building on the preceding findings that established pain’s structural dominance and thematic centrality in the symptom discourse network. To determine whether this prominence reflects general emotional salience or a unique structural role, we examine centrality metrics of pain relative to two core emotion terms: fear and nervousness.
Table 1 summarizes the results of this comparison. Across all three centrality metrics—degree, betweenness, and eigenvector centrality—pain exhibited markedly higher values. For example, its degree centrality (0.821429) was more than six times greater than the highest value in the fear group (0.0937), and substantially higher than the top score in the nervousness group (0.1297). A similar pattern was observed in betweenness centrality (0.930134 for pain versus ≤ 0.2025) and eigenvector centrality (0.695893 for pain versus ≤ 0.3426).
Table 1 Centrality metrics of pain compared to fear- and nervousness-related terms. Columns: metric type (degree, betweenness, eigenvector), pain score, maximum scores in fear and nervousness networks, combined mean ± standard deviation for emotion-related terms, and permutation test p-values (n = 10,000). All centrality values range from 0 to 1; higher values indicate greater structural prominence.
Permutation tests (n = 10,000) confirmed that pain’s centrality scores were significantly greater than those observed in either emotion-related group (p pain functions not merely as a frequent or emotionally salient term, but rather as a structurally dominant hub within the symptom discourse network. Its high connectivity and bridging role distinguish it from typical emotion terms, which tend to cluster within narrower affective contexts. This supports the interpretation of pain as a central organizing term that integrates diverse semantic domains.
Stability analysis of centrality measures
This section presents an evaluation of the stability of key symptom-related terms using centrality metrics and their standard deviations, building on the previous structural analysis. Figure 5 provides a comparative visualization of centrality values and their variability for five key terms—pain, headache, burning, discomfort, and ache—across three centrality measures. Each panel in the figure corresponds to a specific metric: Fig. 5a shows degree centrality, Fig. 5b shows betweenness centrality, and Fig. 5c displays eigenvector centrality. Points represent mean centrality scores, while vertical error bars indicate standard deviations calculated from bootstrap resampling.
Fig. 5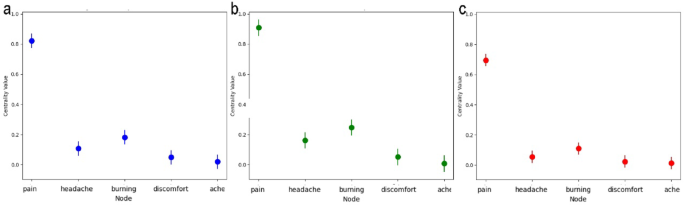
Instability of centrality measures for key pain-related terms. Centrality values and standard deviations for five pain-related terms (pain, headache, burning, discomfort, ache). (a) Degree centrality. (b) Betweenness centrality. (c) Eigenvector centrality. X-axis: node labels. Y-axis: centrality values. Error bars: standard deviations.
In Fig. 5a, pain shows the highest degree centrality with a moderate standard deviation, indicating that it consistently forms a dense set of direct lexical connections across samples. Burning and headache follow with lower scores and slightly higher variability. Discomfort and ache show both low centrality and limited variation, suggesting marginal connectivity and functional specificity in the network.
Figure 5b highlights pain’s role as a semantic bridge, with a betweenness centrality of 0.930134 and substantial variability, reflecting its dynamic positioning across contextual subgroups. Headache displays a standard deviation of 0.161610—greater than other non-central nodes—indicating its context-dependent bridging function. In contrast, discomfort and ache appear rarely along shortest paths between clusters, affirming their peripheral discursive role.
Figure 5c quantifies influence within densely connected regions. Pain again dominates, with burning positioned second in influence but showing a greater variance. Headache, discomfort, and ache all exhibit lower and more stable eigenvector centralities, reinforcing their limited integration into the semantic core of the network.
To further assess the robustness of these findings, 95% confidence intervals (CIs) for degree centrality were calculated using bootstrap standard deviations. Pain had the widest CI (0.193–1.450), underscoring both its dominant and context-sensitive role. Headache showed a CI of 0.020–0.195, while burning ranged from 0.034 to 0.329. Both discomfort and ache maintained lower and narrower ranges, each under 0.090, suggesting stable but structurally marginal positions.
To determine whether centrality variability differs by semantic category, we compared the standard deviations of degree centrality across three lexical groups: pain-related, metaphorical, and emotional terms. Statistical tests revealed that pain-related terms exhibited significantly higher variability than metaphorical terms (Welch’s t = 4.11, p = 0.0052; permutation p = 0.0034), whereas no significant difference was observed between pain-related and emotional terms (p > 0.77). These results suggest that variability is not randomly distributed but reflects functional distinctions within the discourse structure.
Taken together, the centrality stability profiles clarify the structural resilience and contextual adaptability of symptom-related terms. Pain consistently occupies a central yet flexible role, while headache and burning function within narrower, more variable contexts. In contrast, discomfort and ache remain stable but peripheral, contributing minimally to the broader organization of symptom-related language. These findings highlight the importance of incorporating stability metrics into network-based discourse analysis.