- The Utah State Hospital is celebrating 140 years, about half as the state’s only mental health treatment provider.
- Early on, mental illness was often associated with unexpected possible causes, such as epilepsy, poverty and even reading novels.
- Mental health care changed dramatically after 1963’s Comprehensive Mental Health Center Act.
Deer and ducks roam the 312-acre grounds of the Utah State Hospital, resting easily in shade on the beautifully manicured lawn, while neighbors hike, ride bikes and golf on the mental health facility’s property.
It’s a far cry from the state hospital’s isolated beginning in 1885, when it was deliberately located by territorial lawmakers on the swampy land edging the mountain on the east side of Provo, well separated from the heart of the city by a trash dump. Back then, the Utah Territorial Insane Asylum, as it was known, was the only mental health provider in Utah.
This month, as what is now the Utah State Hospital celebrates its 140th anniversary, the hospital is also celebrating how its mission, its place in mental health care and its methodology have all changed drastically.
Deseret News took a tour of the state hospital with its superintendent, Dallas Earnshaw, who started there as a nurse in 1983, and Janina Chilton, now the facility’s historian. For many years, she was the Utah State Hospital spokesperson. When she retired, she stayed on to preserve and share its story.
Wednesday, Utah Gov. Spencer Cox and other officials will help mark the anniversary with the staff, patients and media. It’s a celebration of what’s been learned along the way about providing good care and treatment and the many ways the facility has changed lives for the better.
But alongside successes, there have been missteps, too, Earnshaw and Chilton agree.
Early mental health care in Utah The campus of the Utah State Hospital is pictured in Provo on Sunday, July 17, 2025. | Isaac Hale, Deseret News
The campus of the Utah State Hospital is pictured in Provo on Sunday, July 17, 2025. | Isaac Hale, Deseret News
To say that mental health treatment — and the nation’s understanding of it — has improved is an obvious understatement.
In Utah, the first mental health institution was opened at the mouth of Emigration Canyon in 1869, managed and funded by Salt Lake City. According to Chilton, those deemed violent because of mental illness were put in strong cells there, others housed in very small rooms. That facility would become the Utah Territorial Insane Asylum within a few years when Dr. Seymour Young, Brigham Young’s nephew, leased it. The asylum moved to Provo in 1885.
Perhaps most startling in its history are the reasons people could be committed to the state’s mental health facility, including having epilepsy. The supposed “causes of insanity,” a 67-entry list taken from admission records, is odd by modern standards. It included things like financial embarrassment, disappointment, softening of the brain, death of a child, poverty, jealousy, unreciprocated love, studying prize fighting, ovarian trouble, reading novels, solar heat exposure, overwork, litigation, sedentary life, hypnotism, girl trouble, sheep herder and using cigarettes.
For 85 years, the asylum was the only facility providing mental health treatment in Utah, guided early on by the “Utah State Board of Insanity. ” But in 1963, President John F. Kennedy signed into law the Comprehensive Mental Health Center Act creating robust community centers to treat mental illness. In 1969, Weber Mental Health Center became Utah’s first community mental health center; 13 centers now serve clients statewide. Patients are treated within their communities and those who need more care are treated by one of the centers.
While the Utah State Hospital, as it has been known since 1927, serves a very important role in mental health care, it’s no longer doing it alone. The hospital treats those needing inpatient care because of complex mental illness that cannot be adequately served in the community. Under state law, no one can be committed to the state hospital unless that individual represents a harm to themselves or others. The law says someone must be treated first in a less-restrictive environment in the community. Most people who need treatment for mental illness will never need to be hospitalized.
Introduction of medications called phenothiazines changed everything in the 1950s; in many cases the drugs eliminated psychotic thinking. They unlocked doors to new understanding of how the brain works, exposing the impact of such misfires as overactive or underactive neurotransmitters, which contribute to depression, schizophrenia and other conditions.
 The Utah State Hospital is pictured in the 1960s. | Utah State Hospital
The Utah State Hospital is pictured in the 1960s. | Utah State Hospital
Money helped, too. About the time new drugs were emerging in the ’50s, the Utah Legislature provided new funding and its “forward-looking superintendent,” Dr. Owen P. Heninger, organized the facility into small units with their own treatment teams, a practice that remains.
Many patients were also released back into the community, nearly halving the census from its peak of 1,500 in 1955 to about 800 by the 1960s. Heninger introduced a patient council, ways for patients to earn privileges, a patient newspaper and a family day.
By the end of the decade, families were part of the care team, and they and patients wanted better treatment, better outcomes and alternatives to large state hospitals. They began talking about mental health and addressing stigma. Advocacy and education groups sprang up, including the Mental Health Association and the National Alliance for the Mentally Ill, which have endured and push for research, community care options and fair coverage by insurance.
A fully functioning hospital The Treatment Mall is pictured during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
The Treatment Mall is pictured during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
Over the state hospital’s lifetime, at least five buildings have been demolished and many more have been remodeled or rebuilt on the campus. According to spokesperson Danielle Conlon, the outdoor space has been used for recreation therapy for 75 or more years.
The Utah State Hospital today has 154 forensic, 152 adult and 72 pediatric beds. Many patients are there for months, while very complex patients may stay a long time.
Forensic patients are committed by criminal courts because they require secure inpatient care. They are people accused of crimes who also have mental health or substance use issues. One of the state hospital’s tasks is restoring competency, which means providing treatment to court-ordered adults who need it in order to stand trial.
The campus includes medical clinics, the K-12 Oak Spring School with teachers from Provo School District, adult education, a clothing donation center, library and hair salon, ceramics shop, greenhouse and massive kitchen.
In addition to a large staff, the hospital benefits from more than 800 volunteers who organize activities and fundraisers. The Forgotten Patient Holiday Project is a volunteer-run effort to provide gifts for hospital patients who would otherwise not receive any.
Reading novels and financial worries can no longer send someone to treatment there. Patients have serious mental health challenges. Schizophrenia is common, per Earnshaw. So is bipolar disorder. Patients may have severe depression with complicating factors or borderline personality disorder. “It’s often trauma-based,” Earnshaw said, so great effort is taken not to retraumatize. Physical restraints aren’t used unless absolutely needed. The straight jacket employed through much of the facility’s history has been permanently moved from the supply closet to the museum.
 A digital sign and banner hang along East Center Street on the campus of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
A digital sign and banner hang along East Center Street on the campus of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
The state hospital is proud to have maintained accreditation from the Joint Commission, a nonprofit organization that evaluates health care entities, since 1986. Other facilities within the country often consult Utah State Hospital experts.
Each unit has 40 to 50 employees. Treatment specialty areas include psychiatry, psychology, clinical therapy, music therapy, nursing, occupational therapy, physical therapy, recreation therapy, patient job training and substance use treatment.
The hospital trains hundreds of students, providing internships, student rotations, residencies and postgraduate training in tracks including nursing, psychiatry, psychology, social work, recreation therapy, occupational therapy, physical therapy, chaplaincy and hospital administration.
The geriatric unit is designed a bit like a nursing home, centered around a staff-managed station. How units are constructed makes a difference to care and how well patients do. If the height of the ceilings is too tall, geriatric patients get confused, Earnshaw said. In designing new spaces, the hospital brought in sound experts because patients may have headaches or tinnitus.
With each new building, he said, the staff learned about the mistakes they made in the building before.
If the hospital expands again, it will need a new kitchen; it’s at capacity. They must think about laundry and parking, too. Can it handle more? Administrators have been working on a master plan for the next 15 years.
Halls are bright, but not too bright. They’re clean and have colorful art, but not too much. In one area, there’s a huge painting of Beethoven’s “Moonlight Sonata.” One of the hallways features art with words like “Joy” and “Hope.” During the tour, Earnshaw pointed out one of the facility’s weirdest challenges: deposits left on big windows by water. It is, he said, very expensive to clean.
Although it’s an open campus, patients move around on it with staff or a system of check-ins so at any time, every patient’s whereabouts is known.
Points of pain and pride Janina Chilton, historian of the Utah State Hospital, points out historical photographs in the Utah State Hospital Museum during a tour of the hospital’s campus in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
Janina Chilton, historian of the Utah State Hospital, points out historical photographs in the Utah State Hospital Museum during a tour of the hospital’s campus in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
The history of the state hospital includes many successes. In 1942, it pioneered a change of heart in how to best treat those with complex mental illness, adopting smaller patient units, individual treatment plans and a humane approach. It’s a philosophy now embraced nationwide.
Earnshaw said the Utah hospital was one of the first to study the positive impact of group therapy on those with schizophrenia. It’s the only state hospital to have developed its own electronic medical records specific to an inpatient psychiatric hospital. And not a single patient died during the COVID-19 pandemic.
But its history has low points, even in modern times — and forensics was one reason.
The state hospital was under a settlement agreement from 2017-2022. The Disability Law Center sued over “unconstitutional detainment of prisoners who were sitting in jail cells too long before receiving treatment prior to being proven innocent or guilty,” as Deseret News reported at the time. Patients ordered to the hospital for competency restoration were at the mercy of very long waits, creating the opposite of a speedy trial. Some waited so long they had to be released back into the community, even if it wasn’t a safe option at that time. Under the agreement, the hospital had 14 days to admit such a patient.
It also does a lot of jail-based competency restoration. If competency can’t be restored, a patient may be subject to civil commitment.
Design choices have sometimes led to regret, Earnshaw said. For instance, you have to drive all the way through the campus to find the administration building, which is not helpful for those trying to check in or find their way around.
He added that as the patient population has grown and the illness level has risen, “We wish we could have built units with fewer patients and single rooms.” It’s hard to get lawmakers to fund smaller units, he said.
Another lament? The hospital sold the farm it bought when it needed more land in the 1980s. “We are learning this could have been a more therapeutic opportunity for patients to learn and grow in a natural environment,” Earnshaw said.
He also wishes it had kept better track of reports to show how far it has come in providing care. “We are doing well now but we don’t have data from the past to compare to,” he said, such as length of stay, turnover rates and injury rates.
Chilton regrets the lack of engagement the early hospital had with the community, as well as a dearth of funding early on that led to unsafe, crowded conditions. And some early practices created stigma around those with mental illness.
Museum: A painful look back The central control room for the Forensic Building is pictured during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
The central control room for the Forensic Building is pictured during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News  The library is pictured during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
The library is pictured during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News  The courtyard of the Rampton II Building is pictured during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
The courtyard of the Rampton II Building is pictured during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News  Photos of past superintendents hang in the Heninger Administration Building during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
Photos of past superintendents hang in the Heninger Administration Building during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News  The physical therapy room is pictured in the Rampton II Building during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
The physical therapy room is pictured in the Rampton II Building during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News  Signage for Oak Springs School is displayed during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
Signage for Oak Springs School is displayed during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News  Banners hang along East Center Street on the campus of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
Banners hang along East Center Street on the campus of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News 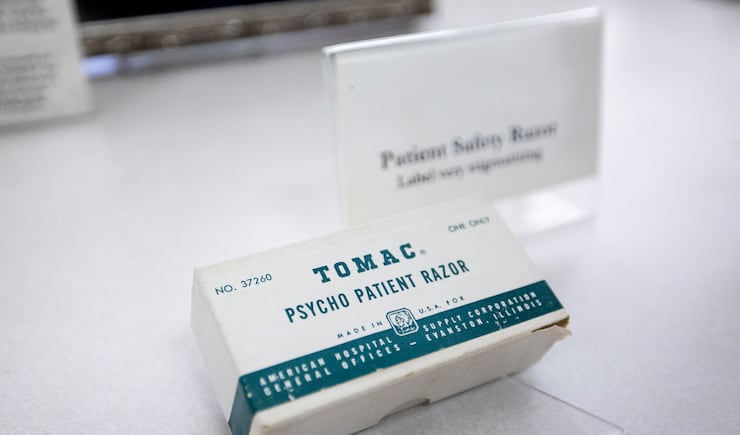 A patient safety razor is displayed in the Utah State Hospital Museum during a tour of the hospital’s campus in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
A patient safety razor is displayed in the Utah State Hospital Museum during a tour of the hospital’s campus in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News  Photographs and items about patient labor are displayed in the Utah State Hospital Museum during a tour of the hospital’s campus in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
Photographs and items about patient labor are displayed in the Utah State Hospital Museum during a tour of the hospital’s campus in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News  Historical items are displayed in the Utah State Hospital Museum during a tour of the hospital’s campus in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
Historical items are displayed in the Utah State Hospital Museum during a tour of the hospital’s campus in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
The history of the state hospital is written boldly on the walls and in the displays at the museum, a building built by the WPA in 1934 that’s on the National Register of Historic Place. The museum doesn’t sugarcoat mistakes but points with pride to its successes.
For its first seven decades, the institution provided mostly custodial care — a place to be, often far away from family. “Therapeutic care was almost unknown in those early years,” per Chilton.
The intake form from a 100 or so years ago now seems somewhat comical, but was written without humor. It asked if a prospective patient had a “homicidal, suicidal or incendiary disposition?” “Is there a disposition to filthy habits, destruction of clothing, furniture, etc?”
Some of the museum’s items are primitive, even nasty by today’s standards. There’s the Utica crib, a long narrow box with heavy wood slats and a locking lid. People having seizures were sometimes placed in it, as were those needing restraint. The Oregon boot prevented someone from moving fast or escaping. Created for Oregon prison warden J.C. Gardner, the device was what Oregon’s historical website calls a heavy steel split cylinder joined about an inmate’s ankle and supported by a stirrup under the instep in very painful fashion. The thing weighed up to 25 pounds and soon became popular not just in prisons, but in facilities for those with mental illness. There were other devices that now would be considered punishment, not treatment.
Feet went through holes in the bottom of the tranquilizer chair and a patient’s head went into a boxlike structure with latticework. With a patient’s feet in hot water, hospital staff would pour cold water onto the top of the head. The box was also used to limit movement, Chilton said, noting the designer believed if someone was agitated the blood would flow from the brain to extremities. He thought if you could limit movement the blood would flow normally back to the brain.
“It was, of course, total nonsense but he was at least thinking about a cause,” Chilton said.
Until 1919, some patients were placed in a cage.
There were also early treatments that later improved. In 1934, the state hospital started using convulsive therapy prompted by a drug. In 1947, a safer form, electronic convulsive therapy, was used. When medications were developed in the 1950s, the hospital stopped convulsive therapy.
In the 1950s, the word insanity was removed from that governing board, the Utah State Board of Insanity. “A lot of what we hate about our history was from them,” Chilton said.
To the future A deer stands in an apple orchard during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
A deer stands in an apple orchard during a tour of the Utah State Hospital in Provo on Thursday, July 17, 2025. | Isaac Hale, Deseret News
Chilton notes that an “arbitrary distinction between physical illnesses and mental illnesses is becoming unnecessary. The positive aspect of this is it allows us to apply the same advanced technology toward solving the mysteries of mental illness that we would to any other form of illness.”
As people within its care have moved back into connection with others, so has the hospital. As Chilton wrote in the history, “That garbage dump is now a park, the swamp has been filled and homes and a water park now surround the campus.”
Hope remains for a cure for mental illness. Research suggests that’s a real future possibility.