The pathophysiology of BBS is thought to be caused by or involve at least 28 distinct genes. The condition’s underlying genetics are complicated. Numerous protein products derived from these genes support the integrity and functionality of the BBSome, a structure essential for the structure and function of primary cilia [7]. The BBS phenotype develops gradually over the first 10 years of life. Consequently, the majority of patients are diagnosed in late childhood or early adulthood [8]. The average age at diagnosis was 9 years [9]; however, this patient presented at the age of 30 years, which is unusual.
Early diagnosis facilitates anticipatory guidance and can be particularly beneficial in preventing or mitigating the onset of obesity. Whole-exome sequencing is currently the first diagnostic test used for patients with numerous congenital abnormalities. However, this patient has been treated in a limited setting, making genetic sequencing not possible. Therefore, Beales criteria are used to diagnose the patient. The diagnosis of BBS requires at least four major features or three major features and two minor features [9]. This patient had five out of six major criteria and one minor criterion, confirming BBS. Table 5 presents the major and minor Beales criteria.
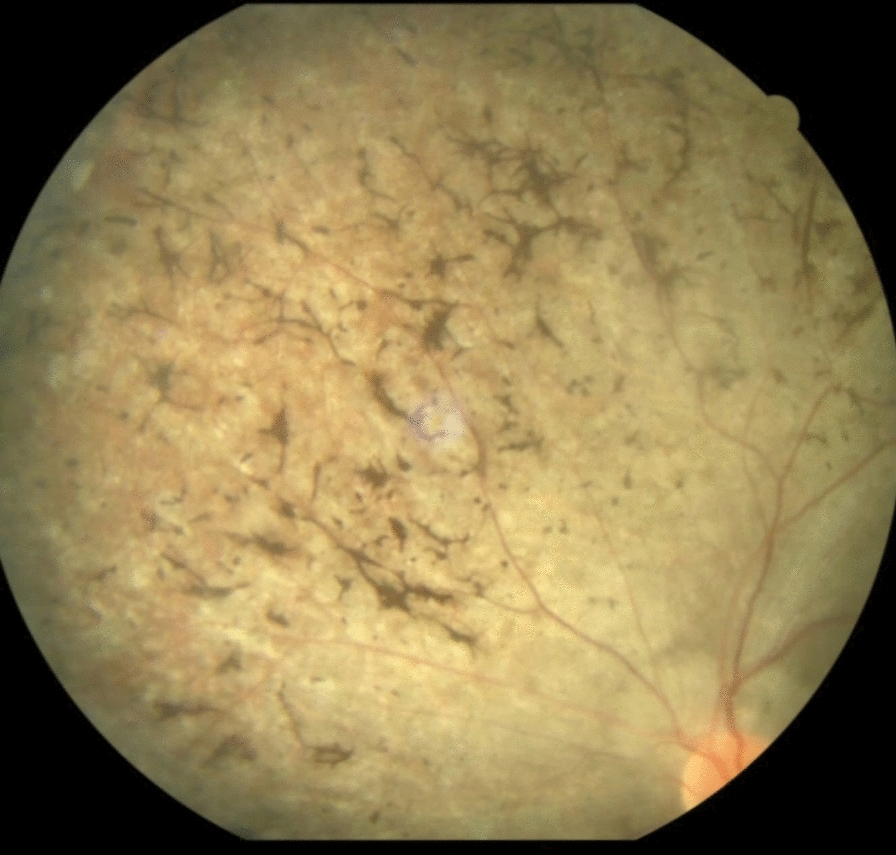
Obesity is estimated to affect 72–86% of people with BBS [10]. In general, birth weight lies within the normal range, and weight gain frequently starts in the first few months and years of life [11]. Childhood obesity has typically been characterized as having a broad and nonspecific distribution. However, by adulthood, the trunk and proximal portions of the limbs exhibit the most evident adiposity. This patient presented in adulthood and was unable to provide a childhood history. However, the most significant sign of BBS is still rod-cone dystrophy, which is present in 90–100% of cases. In BBS, visual impairment has always started early, usually between the ages of 8 and 9, and by the third decade, 98% of patients had lost all of their vision. This patient was completely blinded by the age of 9 years from retinitis pigmentosa. Myopia, astigmatism, strabismus, cataracts, color abnormalities, and retinal degeneration are among the additional visual characteristics [12].
In total, 30% of patients also have liver disease, which is defined as abnormalities in liver imaging and/or high levels of plasma transaminase enzymes; other gastrointestinal abnormalities, such as Hirschsprung’s disease, celiac disease, inflammatory bowel disease, anal stenosis, and other anatomic anomalies, are more common than one might expect in the general population. Patients also had sensorineural hearing loss and hormonal manifestations such as metabolic syndrome, diabetes mellitus, hypothyroidism, and polycystic ovary syndrome [13]. Children with BBS often experience developmental delays in all domains, including gross motor, fine motor, and speech/language. Yet, most of them eventually reach significant developmental milestones, such as walking and talking [14]. They may experience a delay in reaching developmental milestones due to mental retardation or eyesight impairment. This case has suffered from cognitive impairment, leading to difficulty in completing his education.
In addition, 25% of people with BBS die by the age of 44 years, indicating significantly lower survival and longevity. The most frequent and common cause of death is renal failure. A study found that chronic uremia accounted for 38% of deaths, and renal impairment was present in 38% of patients at the time of death [15]. This patient had normal kidney sizes on ultrasound but had a renal cyst in the right kidney. He also had elevated creatinine levels, indicating renal manifestations of BBS. With the early onset of blindness, obesity, hypertension, and diabetes mellitus, Bardet–Biedl syndrome has a poor prognosis.
BBS is treated symptomatically and includes routine screening and monitoring for associated conditions such as obesity, renal abnormalities, and vision problems. Patients benefit from nutritional counseling and weight-management strategies. Ophthalmologic care for vision issues and nephrology evaluation for kidney abnormalities in adults is suggested [16]. Patients may receive surgical interventions for specific complications such as polydactyly, scoliosis, and urogenital malformations.